¶ Label Assignment
EMBED contains the clinical and imaging metadata for hundreds of thousands of screening and diagnostic breast imaging exams, so labels can be assigned in innumerable ways. This can be very complex, but at its simplest, there are two columns that are commonly used to assign labels:
-
BI-RADS Assessment:
Theassescolumn indicates the BI-RADS assessment assigned to a finding. BI-RADS assessments are given as letters (their numeric equivalents are shown below)
Table 1: BI-RADS assessments and descriptionsLetter Number Description A 0 Abnormal N 1 Negative B 2 Benign P 3 Probably benign S 4 Suspicious M 5 Highly suggestive of malignancy K 6 Known biopsy-proven malignancy -
Pathology Group:
Thepath_severitycolumn indicates the most-severe pathology result matched to a finding. These pathology results have been summarized into the following groups by a breast pathologist (taxonomy of pathologies assigned to each category can be found in Figure 5 of the EMBED paper).
Table 2: EMBED pathology group severities and descriptionsSeverity Abbreviation Description 0 IBC Invasive cancer 1 ISC In-situ (non-invasive) cancer 2 HRL High-risk lesion 3 BLL Borderline lesion 4 B Benign lesion 5 NBC Non-breast cancer
¶ Clinical Pathway
The clinical pathway for breast cancer screening and treatment (shown below in Figure 1) should be kept in mind whenever one is approaching label assignment in EMBED.
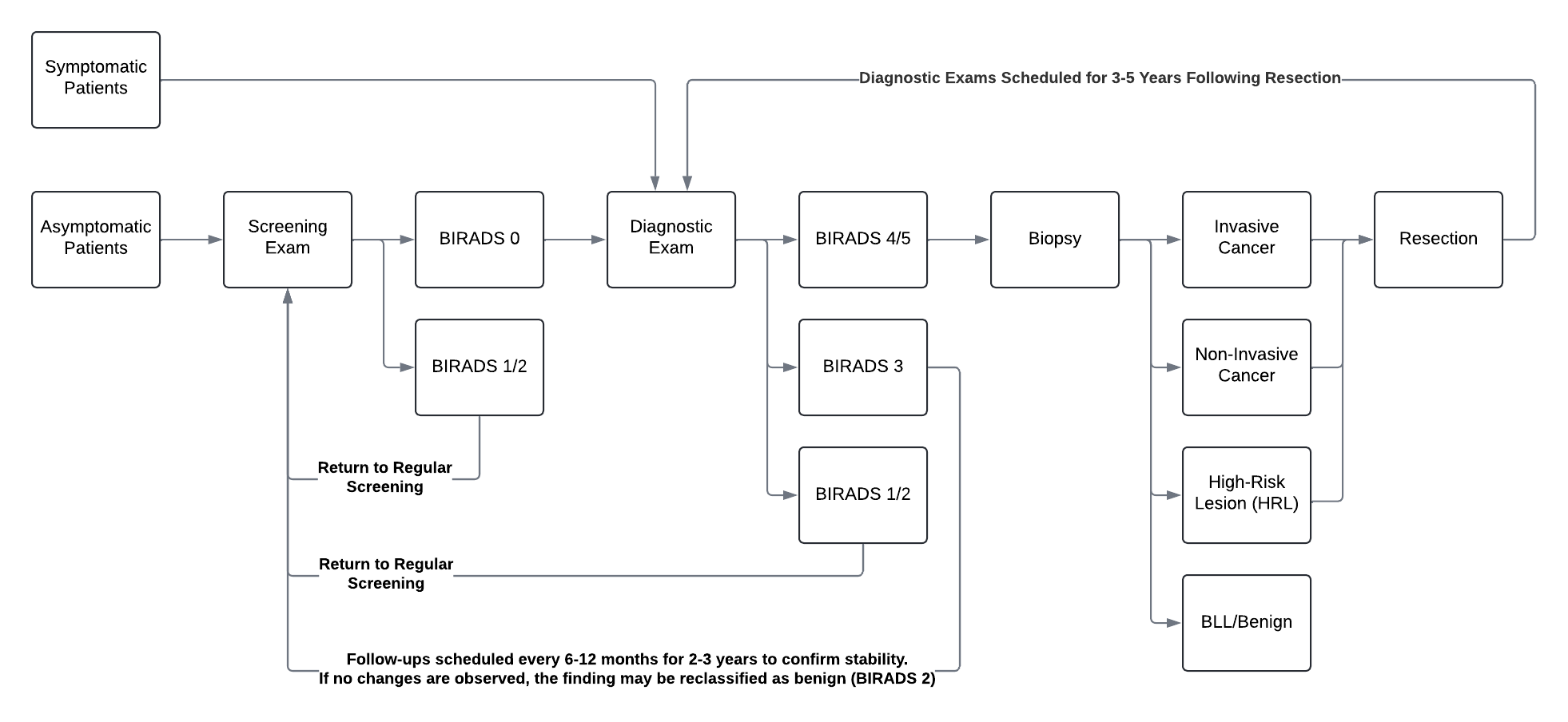
Figure 1: Diagram of the clinical pathway for breast cancer imaging exams at Emory
¶ Screening vs. Diagnostic Exams
As shown in Figure 1, exams are either screening or diagnostic.
- Screening exams are used to identify potentially abnormal lesions which can then be inspected in-depth during diagnostic exams. In the USA, women over the age of 40 are recommended to receive yearly breast cancer screening exams (Emory breast screening recommendations) so developing cancers can be caught early.
During screening, findings can receive a BI-RADS assessment of 0 (abnormal), 1 (negative), or 2 (benign). Approximately 90% of screening exams are negative or benign (BI-RADS 1 or 2), while the remaining 10% are abnormal (BI-RADS 0) and receive a recommendation for diagnostic follow-up. - Diagnostic exams are used to determine the likelihood of malignancy for an abnormal lesion. These generally take place after a screening exam receives an abnormal (BI-RADS 0) assessment, but patients who are admitted for some type of symptom (for example, pain or a mass in the breasts) will go straight to a diagnostic exam.
During diagnostics, findings can receive a BI-RADS assessment of 1 (negative), 2 (benign), 3 (probably benign), 4 (suspicious), or 5 (highly suggestive of malignancy). Approximately 2/3 of diagnostic exams are negative or benign (BI-RADS 1 or 2), with approximately 1/3 receiving a BI-RADS 4 or 5 and a biopsy recommendation. BI-RADS 3 accounts for a very small proportion of cases with specific findings that merit monitoring but no biopsy.
Approximately 2/3 of biopsy results are benign, and the patient will return to annual screening. The remaining 1/3 are malignant and prompt further imaging (MRI to evaluate extent of disease) and/or surgical resection (lumpectomy or mastectomy). Patients who have undergone resection will receive diagnostic exams for several years to monitor potential recurrences.